
As a preface to this, I should include some all-encompassing points with which to contextualize this post:
- I am not an epidemiologist, I have no training in epidemiology.
- I am not a virologist or infectious disease expert.
- The pandemic circumstance requires an incredibly wide consideration of factors and nuance that is not explicitly noted in this post, but should always be kept aware of.
- Essentially everyone should expect to be exposed, at some time in the future, to this virus; whether by natural infection or (hopefully) vaccination.
Where We Are
Being in BC I feel so fortunate to be getting regular communications and leadership from Dr. Bonnie Henry and Minister Adrian Dix. The communications are transparent, measured and objective.
Given the current phase of this pandemic, at least in BC, we are still very much in the acute phase. The focus is on ensuring sufficient hospital and critical care capacity for cases that are most likely due to exposure one or two weeks ago. The social measures: shutting of non-essential businesses, closing of common spaces, physical distancing efforts, etc, are all designed to “flatten the curve”.
The entire purpose of the current measures is to spread out the, essentially inevitable, infections over time. This will:
- lower the peak infection rate, and instead spread them out over time.
- provide time to increase that ‘healthcare system capacity’ line by creating ICU and hospital capacity.
If we avoid overwhelming our healthcare capacity, we can also reduce the number of people who actually die from this disease. Instead they can be appropriately treated and/or hospitalized, develop natural immunity and live out the rest of their lives.
The obvious question that many come to, and is perhaps amplified by our community-wide cabin fever is,
how long do we have to live this way?
The Proposal
Like any control system we require inputs from an outcome we hope to control. We also need an output that can be varied depending on how well controlled our outcome is. A common control system of this sort is known as a Proportional-Integral Derivative(PID) loop controller. It essentially modulates our output, based on how far our input is from the desired value. So, lets set some numbers.
In this case, our outcome that we want to measure is, the percentage of our hospital and particularly ICU capacity that is being utilized. After all, this is the whole purpose of all of our current interventions. This will become the input of our PID equation.
The output, essentially our brakes on this public health vehicle, are all of the social distancing measures, business closures, public space closures, etc. Ideally a control output would be analog. However, for the sake of feasibility we can use a scale to produce a stepped output. Say, for example, ten steps of interventions from most restrictive to least.

- Step 10 interventions – most restrictive option
- eg, ‘lock down’, enforced with fines, etc
- steps 9 through 2 — gradually less restrictive
- step 1 – least restrictive
- perhaps continued reminders from health authorities to encourage distancing, hand-washing and no massive group gatherings.
The process could work something like this.
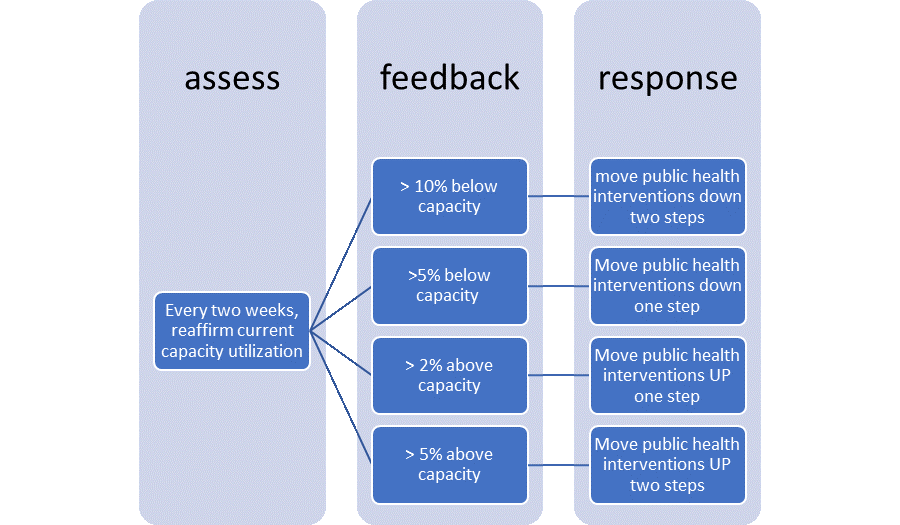
Set a target setpoint of, say, 50% ICU/Hospital utilization for Covid patients. The response to these measures then could be per the process below (numbers are quite arbitrarily set). Note the more amplified inverse response to being above capacity, compared to being below.
As we know the lag from infection to symptom manifestation can be up to two weeks, this seems an appropriate amount of time to assess how the changes to the interventions have affected infection rates. This also ensures we aren’t making changes too often, leaving people unsure of where we are at.
End Point – Herd Immunity
In addition to this grossly simplified proposal for this maintenance phase of our local pandemic, we need to monitor for an end point. We know that virtually everyone will eventually be infected, the only point in this whole process is to slow that eventuality’s arrival to ensure sufficient healthcare is available as we discover who will become severely ill as a result.
Thus, we need testing. Specifically, we need antibody testing. If carried out strategically, a randomized sample of population antibodies could be taken monthly. A sampling of a relatively small randomized sample each month could be sufficient to get a reasonable estimate of overall population natural immunity. This would then allow us to add nuance to the above process as we near a ~80-90% immunity level in our local population. This very well may occur well before a vaccine even becomes available.
Special Consideration
Of course, within all of this, there are significant groups in our population that require outsized protections that would not be well served by this blanket response. We know persons with pulmonary disease, cardiac disease, immunodeficiency, obesity are at significant risk of death from Covid-19. Public policy needs to recognize this and ensure that these folks have particular attention paid to their social and financial needs until a vaccine is approved and available.
Once available, these folks should be first to receive it, as it’s known exposure dose will make it a much safer way to gain immunity compared to unknown viral loads received in the community.
Summary
This is not easy, and no one knows what is the best approach to balance the safety of our population while enabling those that can to safely continue to provide services our communities need and support their families and the economy.
What I hoped to present here was a simplified option to accomplish this, which also would enable for transparency to everyone in the community why particular lockdown measures were in place and why they were shifted to more or less restrictive degrees. Seeing this relationship would hopefully allow buy in from everyone in our province as they would see the consequences of not observing the measures, and also would see the light at the end of the tunnel and how we can get there. Every two weeks we would receive an update from Dr. Henry and Mr. Dix accompanied by:
- current hospital and ICU utilization by Covid patients in %
- which rung of the public health interventions response we are on, 10 – 1.
- a breakdown of what the measures on our public health interventions rung includes
- last measured antibody testing sample, and the extrapolated population immunity
- new forecasting based on this date
I am not an expert in this area and welcome any discussion on the content as you might have.
