
“after morning rounds we need to be sure to get prepared for afternoon rounds, so that we don’t run late into handover rounds”
~ me
This was my most intimidating elective thus far. Everyone involved is so dialed in. Nursing is 1:1 and so knows the patient better than anyone. Each patient has their own Respiratory Therapist (because what are you doing in the ICU if you are not intubated?) and the Intensivists can rattle off all the most recent literature as though it were just another word in the dictionary.
In keeping with this environment, my two fellow medical students were impressive. They would read around their patients ahead of time, linger well after shift to see what could be learned and always had quality patient presentations.
The side effect of being surrounded by this keenness, hopefully, was to push me during the rotation as well.
My ICU rotation at a major centre in Metro Vancouver.
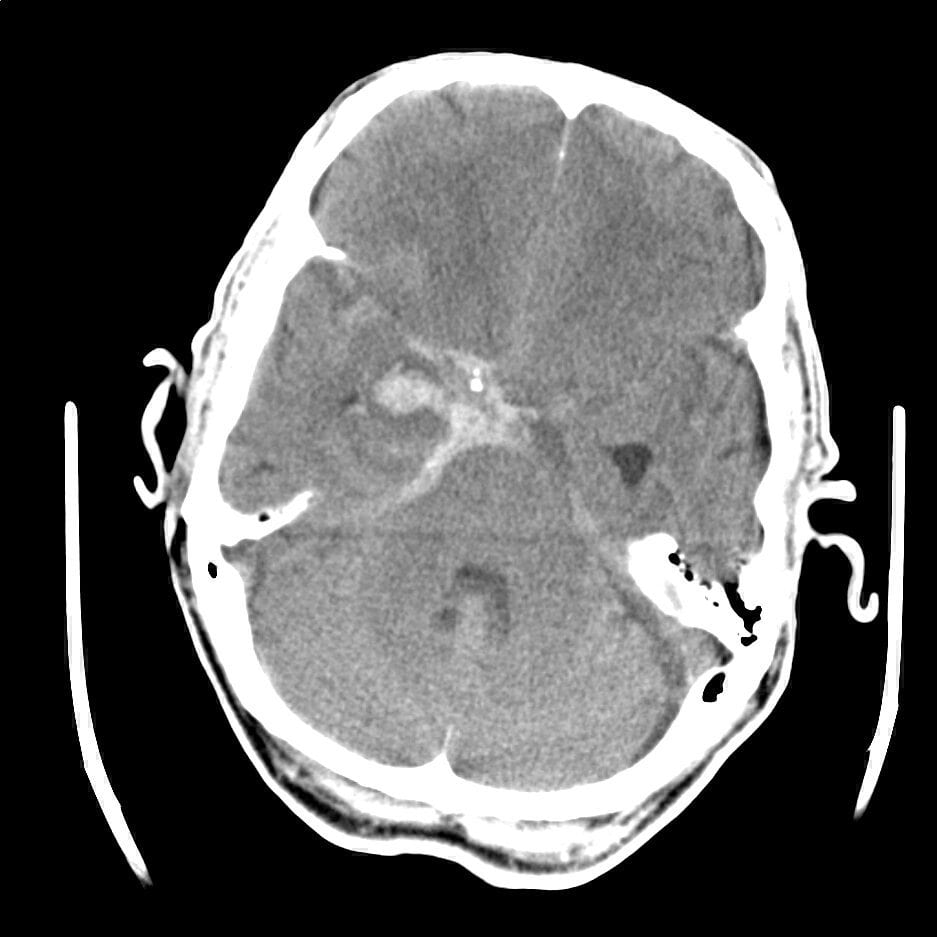
My very first case was doled to me first-thing on day one. A subarachnoid haemorrhage. This had progressed quickly to a decreased level of consciousness in the ED and so follow-up CT-A was done to observe the vessels. There were multiple areas suggestive of vasospasm, a common occurrence in these cases, and also a bad complication.
The solution with vasospasms is Nimodipine regular dosing, and pushing up their Mean Arterial Pressure(MAP) in 10mmHg steps until their level of consciousness improves. The theory is easy to understand. The vasospasms are blocking flow of blood into the brain, push up the blood pressure until there is evidence that the flow is sufficient and keep in there. Repeat CT-angiogram of the head to confirm resolution and we can begin to allow the blood pressure to fall back to physiological norms.
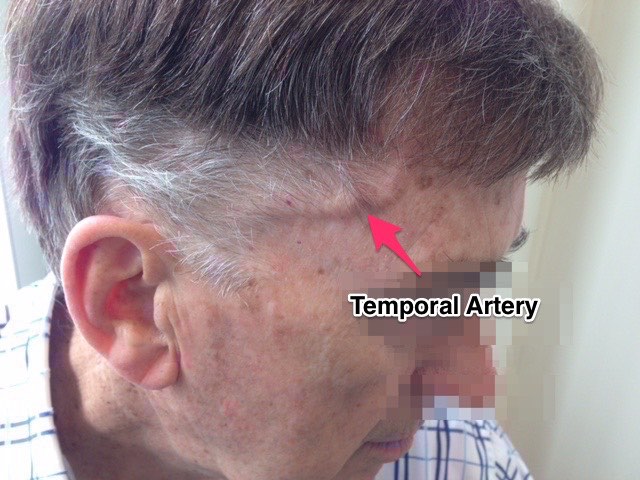
A second patient was added onto my coverage for the second day. This one was also decreased LoC. However, this time the cause was, what seemed to be, a classic case of Giant Cell(Temoporal) Arteritis. However the presentation was very delayed and it had progressed to where she had lost consciousness.
Giant cell arteritis is most common in women 40-60 years old and often presents with pain when chewing, tenderness along the temple and can begin to affect vision on the affected side. If discovered a biopsy of the artery is taken and treatment is most often a short cycle of steroids to calm the inflammation within the blood vessel.
This case however, was so severe that the patient essentially developed stroke symptoms. She was dosed with multiple days of a much more powerful steroid in the ICU and she began to recover. She did so well that we were able to extubate her and even began the process of lining her up for neuro-physiotherapy and rehab. She was stepped down to the HAU but unfortunately had to be brought back and the process restarted again, this time with the addition of immunomodulators.
This case was incredible and gave me a new found respect for the condition, as all other cases I had seen were readily treated as an outpatient from the Emergency Department.
The other aspect of ICU are ED consults. I had a few during my overnight call shifts. Many of which I felt surprisingly comfortable doing the assessment independently. I think the Trauma elective in South Africa was very effective in preparing me for essentially anything that might come through the doors. Of course for us, it is comforting to know that the Emergency Department has already mostly stabilized the patient as needed by the time we are down to see them and admit.
The first three weeks of the rotation it was only us three students, two residents and the consultants. This was amazing as it meant more patients, more procedures and tons of one-on-one time with the consultants. It also meant we were grilled multiple times per day about our patients and their management. In addition, overnight call meant you were often seeing the patients yourself, taking pages, and then confirming your plan with the resident or consultant before trying to sneak in an hour or two of sleep. No diffusion of responsibility where there are only three of you.
The last week we came in to find EIGHT new residents for morning handover. Of course it was great to meet so many wonderful people and learn from them. The difference however was that we suddenly only had one patient per day. There was not enough grilling to go around, and there were many fresh residents hungry for procedures. This made me appreciate that we had the three weeks or relative independence we had enjoyed.
I had little expectation for ICU, but I have to say I really enjoyed it. You are the last line for the sickest of the sick, the inter-professional teamwork and collegiality is second to none, and the medicine is involved and nuanced with tons of procedures as your competency allows.
An EM -> CCM fellowship wasn’t really on my radar until this rotation, but now it might very well be on my list. Rounds and rounds it goes…
